See eicosanoids
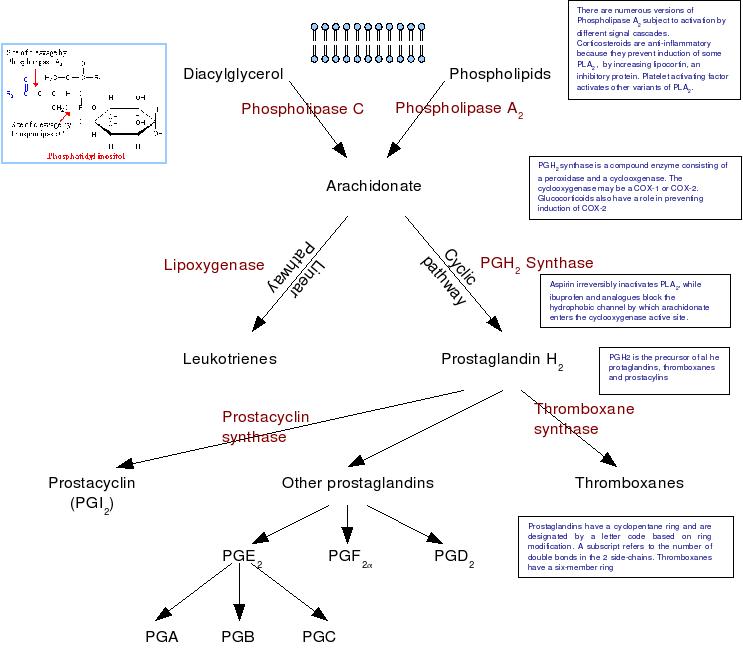
Essentail fatty acids (of which arachidonic acid is the most important) are metabolized through oxydative pathways to form a number of biologically active mediators, including prostaglandins, protacyclins, thromboxane, slow-reacting substance of anaphylaxis, leukotirenes and other simple monohydroperoxy and monohydroxy fatty acids.
All of these compounds are rapidly degraded in the liver, kidneys and lungs and so have an effect only in the immediate vicinity of their site of production. Prostaglandins are not stored and release equates to de novo synthesis. Under normal cicumstances,, prostaglandin production is almost zero, but sysnthesis can be activated within seconds of a hormonal or pharmacological stimulus. The liberation of free arachidonic acid from phospholipid stores is the event whihc triggers prostaglandin synthesis (and consequently, any trauma also triggers prostaglandin production).
They have roles in inflammation, fever, regulation of blood pressure, clotting, immune modulation, control of reproductive processes, tissue growth and regulation of the sleep-wake cycle.
Two isoforms of PGH2 synthase exist, both of which are bound to the endoplasmic reticulum.
COX-2 inhibitors are anti-inflammatory and are less likely to cause gastric irritation, but the is an increased incidence of cardiovascular incidents. This may be attributed to:
Cyclooxygenase is found in almost all animal tissue, whereas the enyzmes which convert PGH2 into other products are far more localized, so in platelets, almost all of the PGH2 is converted into TxA2, whereas in the endothelium, the products is prostacyclin (PGI2) and in mast cells PGD2.
PGD2 on DP-receptors causes vasodilation, inhibition of platelet aggregation, relaxation of GI muscle, uterine relaxation and modification of the release of hypothalamic and pituitary hormones. Signal transduction involves adenylate cyclase and an increase in cAMP.
PGF2α on FP-receptors causes myometrial cntraction. Signal transduction ivolves InsP3 prodution and an increase in cytosolic Ca2+.
PGI2 on IP-recptors produces vasodilatation, inhibition of platelet aggregation, renin release and natriuresis via effects on tubular reabsorption of sodium. Signal transduction involves adenylate cyclase and an increase in cAMP
TXA2 on TP-receptors causes vasoconstriction, platelet aggregation nd bronchoconstriction. ignal transduction involves InsP3 generation and increasing cytosolic [Ca2+]
PGE2 are as follows:
Mast cell activation results in a burst of arachidonic acid metabolism via both the cyclooxygenase and lipooxygenase pathways. Both the leukotrienes and prostaglandins are mediators of local vasodilatation and increased tissue permeability. The leukotrienes C, D and E (formerly categorised as the slow-reacting substance of anaphylaxis - SRS-A) are probably a mediator of bronchospasm in asthma.
TxA2 is a very potent promoter of platelet aggregation, while prostacyclin PGI2 opposes its action. At low dose, aspirin is relatively selective in blocking thromboxane A2 synthase and this coupled with the inability of platelets to regenerate inactivated cyclooxygenase favours an potent anti-throbotic effect.
Renin secretion is regulated by catecholamines and prostaglandin pathways. The latter is activated by a fall in renal arterial pressure and a change in the salt balance in the ascending limb f the loop of Henle. Renal prostaglandins may regulate renal blood flow and GFr in patient with severe heart failure and as a result, cyclooxygenase inhibitors may trigger an acute deterioration in renal function.
Under surgical conditions, arachidonate metabolites are released n large quantities and probably become an imortant factor in the control of local blood flow.
Becuase the eicosanoids have such disparate and local actions, therapeutic use tends to be limitted to sites in which local application is possible, otherwise marked side effects are common (nausea, vomiting, diarrhoea, flushes, hypotension etc.
Prostaglandins E and F can be used to induce mid-trimester abortions. A suppository of PGE2 (gemeprost) is now the preferred method. At term, PGE2 gel (dinoprostone) can be used to ripen the cervix in preparation for induction of labour. Postpartum haemorrhage can be controled using the 15-methyl analog of PGF2α (carboprost) which stimulates uterine contraction
Prostaglandin production is important in maintaining the patency of the ductus arteriosus. Indomethacin is used to encourage the closure of a patent ductus, whereas in infants with a ventricular outflow obstruction (who are dependent on the ductus) it may be sustained by an infusion of PGE1 (alprostadil).
PGE2 and PGI2 suppress gastric acid secretion and misoprotol, a stable PGE2 anaolog can be used for the management of peptic ulcers.
Epoprostenol, a short acting PGI2 may be infused. It may also be used to treat primary pulmonary hypertension.