Centrally acting hypotensive agents
α2 agonists
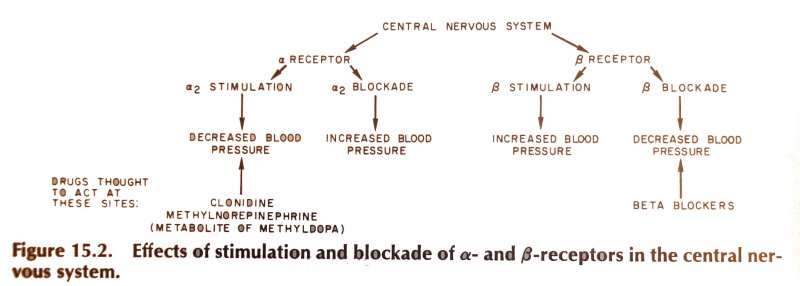
Stimulation of central α2 receptors results in a reduction in outflow of sympathtic outflow and produces a reduction in blood pressure. In addition, plasma renin activity falls, probably as a result of reduced sympathetic stimulatoin at the renal adrenergic receptors. Stimulation of pre-synaptic receptors (which inhibit catecholamine release) may also play a role.
The centrally acting hypotensive agents do not interfere with the sympathetic reflexes (which depend on peripheral adrenergic neurones) and are less associated with postural hypotension.
Clonidine (BNF)
A 'clondine withdrawal syndrome', may occur on abrupt cessation of the drug. It is characterised by hypertension, tachycardia and catecolamine concentrations and may resemble phaeochromocytoma. Clonidine should be re-started, although α-blockers may also be effective in treating the symptoms.
Methyldopa (BNF)
Methydop udergoes decarboylation (L-amino acid decarboxylase) to give α-methyldopamine which is in turn converted to α-methynoradrenaline (dopamine hydroxlase) to α-methylnorepinephrine. This compound stimulates post-synaptic α-2 receptors and reduces sympathetic outflow from the brain.
Particularly at high doses, methyldopa is associatdwith sedation and difficulty in performing compex tasks. These effects may be minimised by taking a once-daily dose at night, allowing the peak sedative effects to work overnight. The peak anti-hypertensive effect is seen 6-8hrs post-dose. The most serius side effect is a potentially fatal hepatic necrosis. All patients must have regular LFT's.